
As if the Pittsburgh Steelers loss to the Miami Dolphins wasn’t painful enough, fans of the team were further dismayed Sunday night as the news broke that QB Ben Roethlisberger sustained a torn meniscus to his left knee and would undergo surgery Monday. The only question on twitter was when would the franchise QB be able to play again. Unless you have been hiding under a rock (and who could blame you after that hot mess in Miami), you’ve heard even beat reporter, NFL insider, and twitter doctor estimate that Big Ben will be out for 2-3 weeks, likely to make his return to face the Baltimore Ravens in week 9. While Coach Mike Tomlin wouldn’t comment on the timeline for his quarterback’s recovery, it seems extraordinarily unlikely that Ben will be under center when the Patriots come to Pittsburgh next Sunday.
So I can’t tell you how long Landry Jones will be the starter, but I can take you through meniscus tears 101. Here we go!
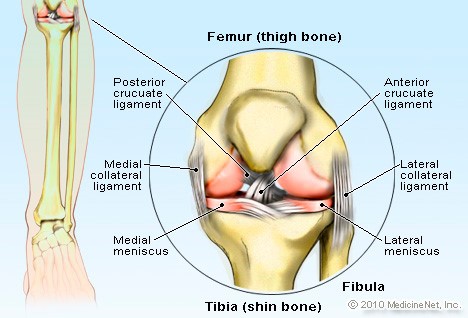
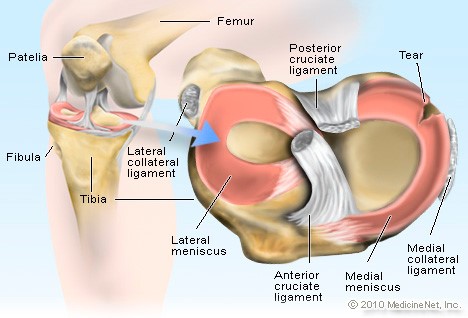
As always, a little anatomy to start. Each knee has a medial and lateral meniscus. These crescent-shaped bands of cartilage serve as the shock absorber for the knee and allow the tibia (the larger of the lower leg bones) to glide over the bottom of the femur (thigh bone) when the knee bends. The menisci are wedges, thicker at the border where the blood supply is best and thinner in the inner aspect, which has a limited blood supply. The lateral meniscus covers a larger portion of the tibial plateau (the flat top of the tibia that articulates with the femoral condyles to form the knee joint).
A tear in the meniscus is usually caused by a quick twist or turn of the knee. As you might expect, this is a common injury in athletes. Older patients can get a tear because the tissue is old and thinned. The mechanism most likely to cause a medial meniscus tear is abduction (the leg bends out away from the body) and external rotation while bearing weight with the knee flexed. A lateral meniscus tear is caused by the opposite scenario, meaning abduction and internal rotation of a semi-flexed knee bearing weight.
With that in mind, look again at the film of Ben’s injury, knowing that he was diagnosed with a lateral meniscus tear. His right foot seems to catch his left foot or ankle, turning it inward as he runs away from a potential sack:
The diagnosis of a meniscal tear can often be made clinically with the following tests (click on the test names for further detail):
- McMurray Test – The patient lays on his back with the knee and hip flexed and the lower leg internally or externally rotated. The leg is then straightened. If the patient feels pain or the examiner feels a click or pop, it is suggestive of a meniscal tear.
- Apley Test – The patient lays prone (face down) with the knee flexed, and the examiner rotates the lower leg. Depending on the motion and location of pain, this test can differentiate between a ligament or meniscus injury.
- Thessaly Test – The patient stands on one foot with the other knee flexed first at 20 degrees, then 50 degrees and rotates the leg internally and externally. If the patient experiences pain or locking of the joint, it is suggestive of a meniscal tear.
A tear of the meniscus is typically described by the orientation of the tear:
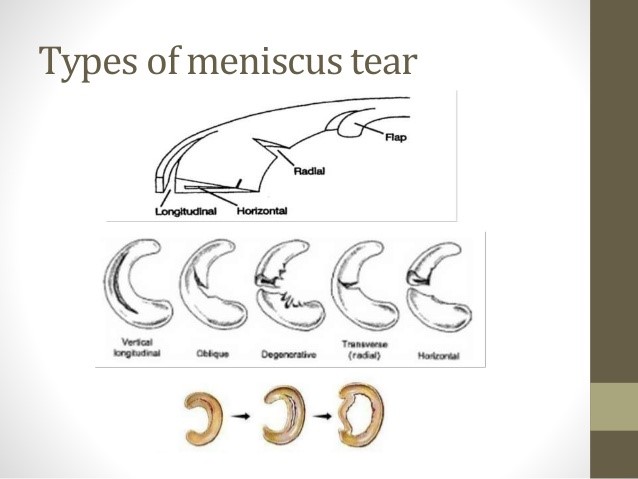
(from a presentation by physiotherapist Khairul Nizam)
Along the bottom of the illustration you will also see an example of a “bucket handle” tear, where the inner border of the semi-lunar cartilage tears away from the peripheral border. This is considered a displaced tear.
As you know, the diagnosis is confirmed by MRI. As far as symptoms go, a meniscus tear can give intermittent locking of the knee as well as swelling and pain, but weight bearing is still possible and does not tend to worsen the pain. This is why Ben was able to return to the game, not that he was playing at the level we have come to expect. Then again, he wasn’t doing that prior to the injury either.
Meniscal tears are typically treated surgically with one of two options:
- Partial or complete meniscectomy (removal of part or all of the meniscus on the affected side)
- Repair of the meniscus
Remember earlier that I mentioned only the outer, thicker border of the crescent-shaped meniscus has a good blood supply and the inner border of the meniscus is avascular? That is a factor in the choice of operation. An attempt to repair the inner rim is usually not successful because the lack of blood supply does not allow for healing the edges of the repair. The type and size of the tear can also make a repair difficult or unlikely to succeed. Based on the type of tear Vikings RB Adrian Peterson sustained, he underwent repair and is currently on IR, hoping to work his way back to the active roster. If you want to really geek out on meniscus repairs, there is a nice review by a group of Germans, one of whom was at UPMC.
If a meniscectomy is the operative plan, the goal is to preserve as much of the intact meniscus as possible. Ben reportedly had a partial meniscectomy, meaning that the torn portions of the meniscus were removed and the edge was smoothed out…what is referred to in the sports news as a “clean up”. This surgery is almost always done arthroscopically, with a few tiny incisions and a telescope to show the inside of the knee on a video monitor.

Here is a video of a surgery very similar to what Ben would have had, courtesy of Dr. David Geier, an orthopaedic surgeon and sports medicine specialist in South Carolina. In the video, you can see the instrument removing the raw edges of the torn meniscus and then smoothing the border with a shaver device. The fragments are all removed from the knee near the end of the procedure. This type of surgery usually takes about 20-30 minutes.
With a partial or even a complete meniscectomy, patients are able to be full weight bearing immediately after the surgery, so no crutches are necessary unless the patient is hesitant to walk due to pain. Pain is primarily due to swelling from the initial injury and tends to be the rate-limiting step to recovery.
OK, I know what you’re thinking: “Hey, Philip Rivers played 6 days after his meniscus surgery, and Big Ben is easily as tough as Rivers, so he is totally gonna play against the Patriots this week!” But slow down for a moment. Yes, it is possible that Roethlisberger could play this week. As a QB, it would be less challenging to play soon after surgery than if her were a WR, RB, or DB. And even if he made his knee more sore, it wouldn’t cause any long term damage. But it could worsen his swelling and delay his recovery, and he might be limited by pain. We’ve all seen the injured version of Ben play, and it hasn’t always been such a great idea in retrospect. Rivers played because it was the AFC Championship, and there was no tomorrow for him if the team lost. That original 2-3 week estimate is a lot more reasonable, especially with the bye week on the horizon.
But is 2-3 weeks realistic for an NFL player? You have probably seen a comment from Dr. David Chao on twitter that lateral meniscectomies take longer to recover than the same procedure on the medial meniscus. This was suggested by a study involving 90 “elite” soccer players; 42 had a partial lateral meniscectomy and 48 underwent partial medial meniscectomy. The author, Dr. Danyal Nawabi, found a statistically significant difference between those two groups in terms of return to pre-injury level of play: 7 weeks for the lateral group and 5 weeks for the medial group, although this is not entirely scientific because he rounded up or down to the nearest week. I wonder what he would have found if he had calculated days instead, which would have been more accurate (or maybe he was massaging the data by picking his parameters to support his hypothesis, which is common in the world or research). He also found that athletes in the lateral group had a higher rate of adverse events (pain, swelling) compared to the medial group.
I couldn’t find any other medical studies on this subject comparing medial versus lateral meniscectomies. In speaking with orthopaedic surgeons, it seems to be a generally known fact based on their experience. But we just happen to have a real life example of an NFL quarterback who underwent a partial meniscectomy for a lateral meniscus tear. EJ Manuel sustained his injury in the second preseason game of his rookie year on a Saturday night 8/16/13 and underwent surgery the following day. He started the Buffalo Bills season opener on 9/8/13 – 22 days later – going 18 of 27 for 150 yards and 2 TDs against the Patriots. By the way, when Philip Rivers played 6 days after his surgery it was also against the Patriots.
We should know more over the next few days, or not, depending on Coach Tomlin’s inclination to continue his pattern of ruling out players early. I would bet that Ben Roethlisberger follows the recovery timeline of EJ Manuel, returning 3 weeks later to face a division rival just as EJ did. In this case, the Baltimore Ravens will be waiting in week 9.
